Mobilising evidence and knowledge bite-size 2
The slides and script from the second bite-size video on Learning Before.
Welcome to the second video in our short series of bite-sized introductions about mobilising evidence and knowledge where we will look in more detail at some Learning Before techniques.
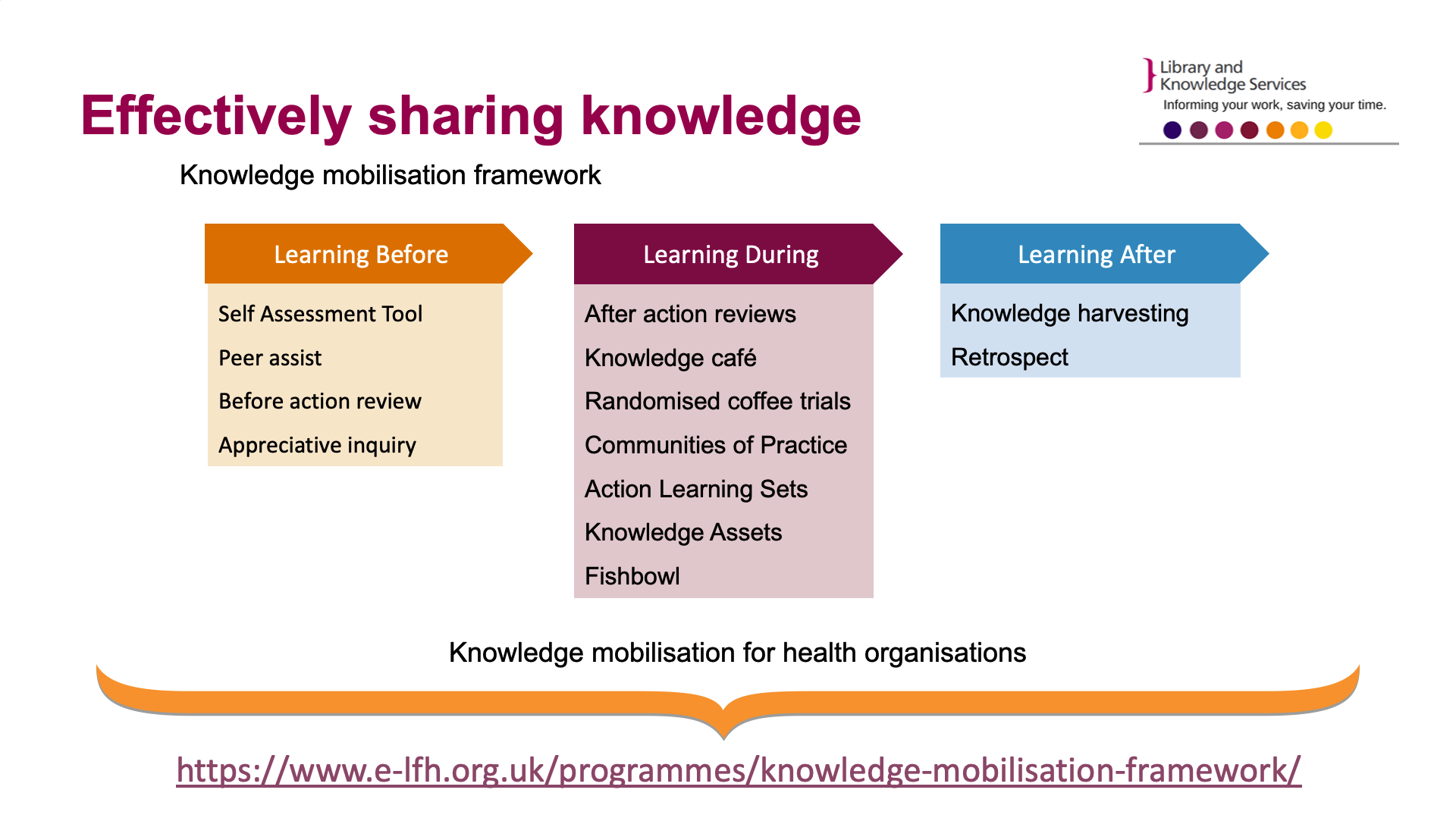
Healthcare is a knowledge based industry. Sharing the know-how of staff, using research evidence and implementing best practice are all business critical. The Knowledge Mobilisation Framework emphasizes learning throughout the an activity’s lifecycle: learning before, during and after. It provides a set of tools and techniques that are simple and quick to use that people can integrate into their daily practice, to encourage continual learning, replication of good practice and avoidance of pitfalls. The tools and techniques facilitate learning and support strategic planning, operational delivery and sustainability.
It is a cyclical process – learning before can lead to learning during and learning after which then feeds back into learning before.
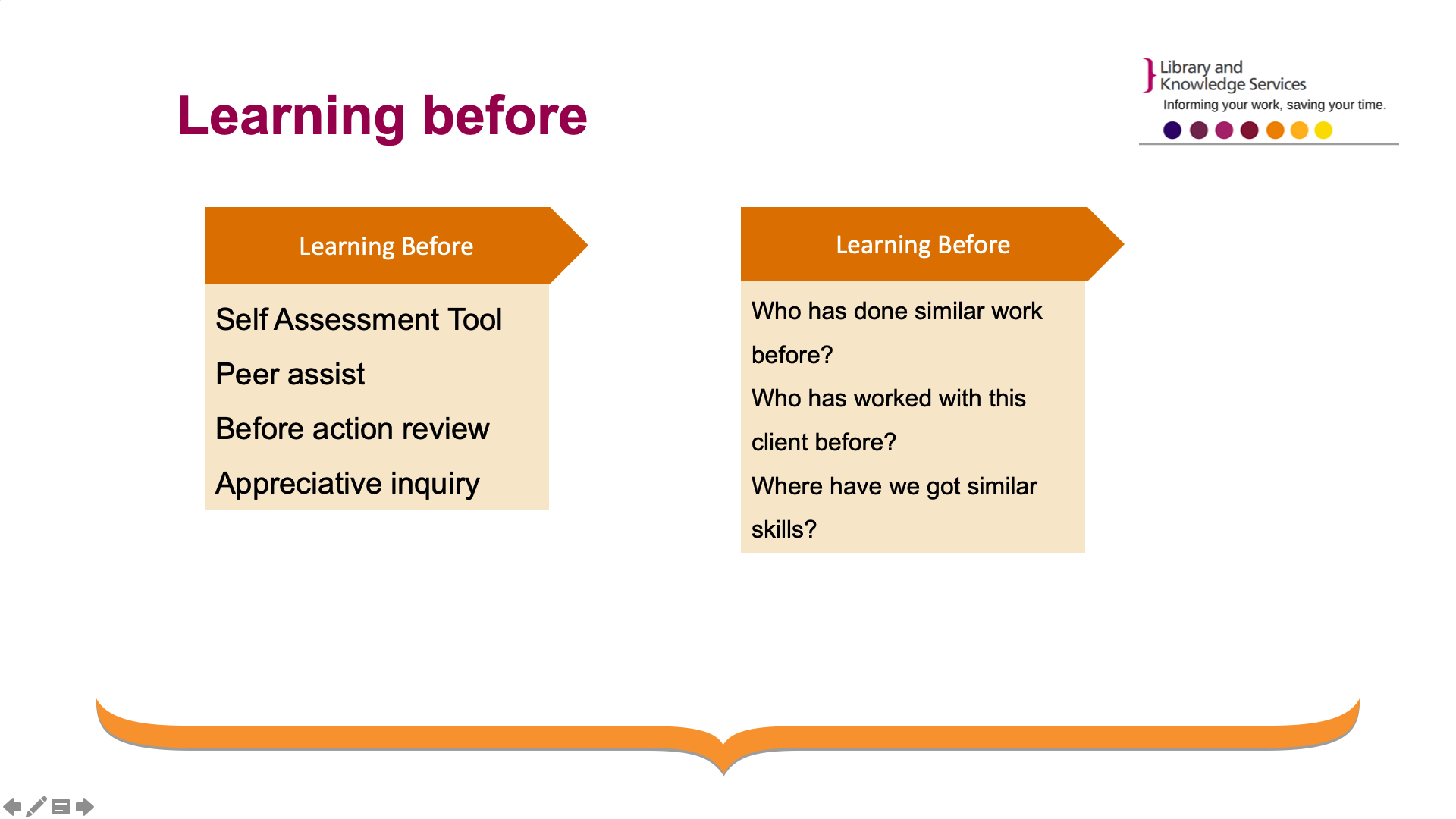
By improving learning before you consider who has done similar work before? Who has worked with this client before? Where have we similar skills?
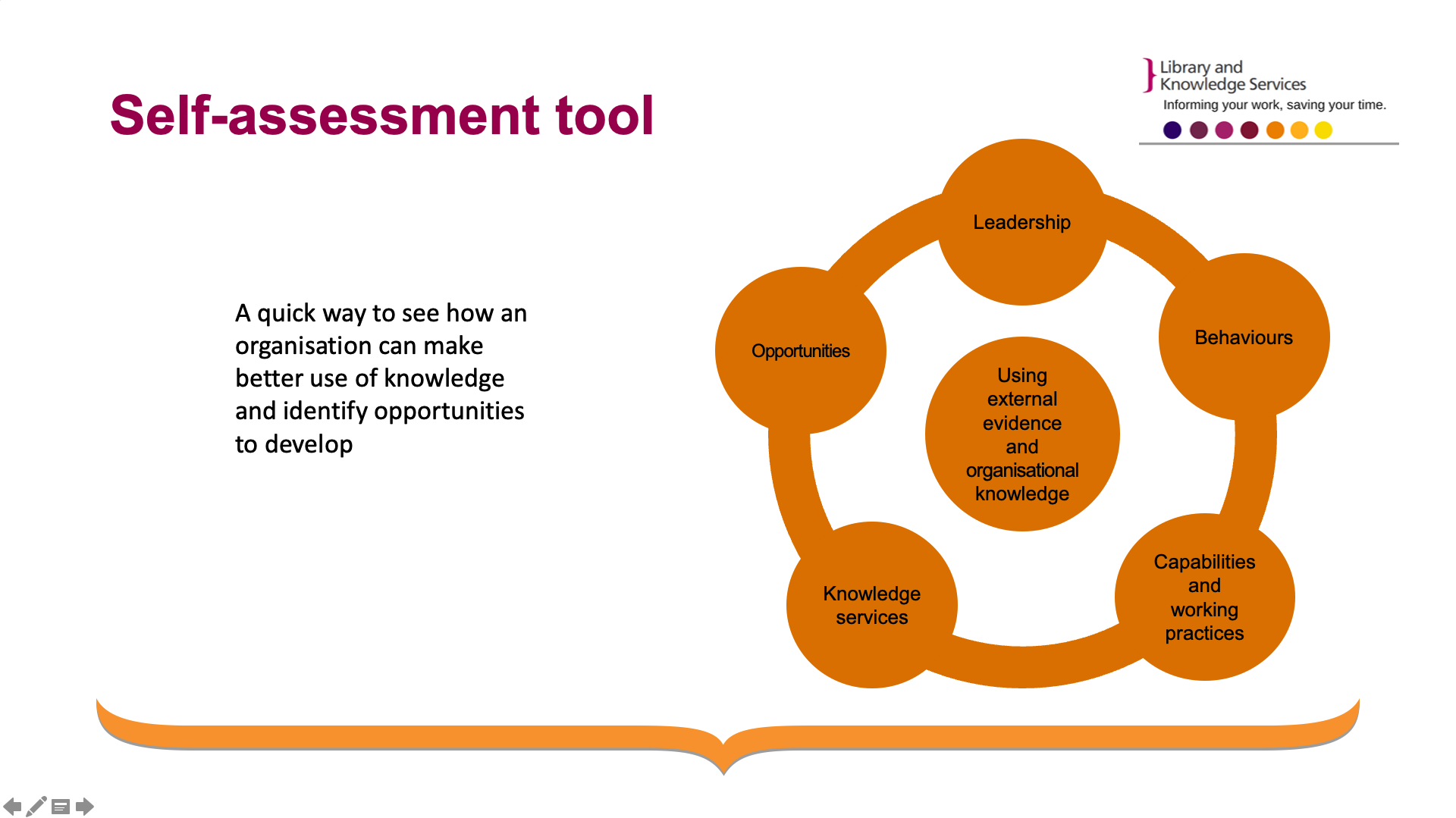
The self-assessment tool is a simple framework has been developed to quickly assess how a team or health organisation can make better use of knowledge as an asset. Often referred to as “The Board Tool” this framework enables a dialogue between a representative of a library and knowledge service and senior executives in a health organisation to see how they are currently using external evidence and organisational knowledge and to devise an action plan to help the organisation develop best practice with targeted support.
The technique takes approximately 1 hour to use and helps to open up dialogue about the range of services the local library and knowledge team can offer to help the organisation meet their objectives.
Rachel Cooke has used the self-assessment tool in her Trust, Surrey and Sussex Healthcare NHS Trust. It has transformed the way her team works with the Medical Division. Rachel says:
“I used the evidence and knowledge self-assessment tool with the Medical Division at Surrey and Sussex NHS Trust. They found the tool easy to use and were enthusiastic about the opportunities it presented. As a result of using the tool a member of my team now regularly attends the Divisional Board Meeting to respond to knowledge and evidence needs that arise during the meeting and act as guardians for ensuring divisional policies are fully evidence based, updated and easy to access.”
A Peer Assist is a structured facilitated meeting or workshop where people are invited from other business units or other businesses to provide their experience, insights and knowledge to a team who have requested help.
Ahead of the peer assist session it is important to appoint a facilitator as well as circulating background information including purpose and objectives of the meeting.
There are four stages to the peer assist.
- The home team present context, history and plans for the future and what they hope to get out of the meeting.
- Visitors ask question and provide feedback about what worked well for them and what could have been done better.
- The Home team analyses and reflects on what’s been learned and examines options.
- Finally, the visitors present feedback answer questions and agree actions with the home team.
The duration of the process is usually half a day. The teams benefit by gaining insight into how someone else has approached something and confirming an approach that was taken.

To see real benefits from a peer assist, view the interview with Professor Martin Elliott a surgeon at Great Ormond Street Hospital. Martin undertakes arterial switch procedures which is an open heart surgery that restores a normal blood circulation in a baby's body. He was concerned that it may be factors associated with the teams involved rather the health of the patient that may adversely impact on the wellbeing of the baby. This procedure normally takes a surgical team 6-7 hours; the baby is then transferred to Intensive Care where it is the responsibility of a new team to manage the baby’s care.
The idea to get in touch with the Ferrari Formula One Team came following a late night and early morning of surgery when a grand prix was on the television in the break room. The pit stops took as little as 6.8 seconds and everyone involved had specific jobs to do and it looked a very slick operation. A colleague of Martin’s got in touch with Bernie Ecclestone who put the team in touch with Ferrari. It soon transpired there was a mutual professional interest in doing something well.
The Surgical team travelled to Marinello to meet the Ferrari F1 team.
The F1 pit stop team have a clear definition of roles and leadership. They rehearse many times verbally and rehearse and try to anticipate what might go wrong. In the NHS there is often little time for rehearsal.
On returning to the UK the surgical team brought in a human factors expert who conducted and observational study which resulted in a number of interventions including structured handovers, defined tasks and rehearsals. The result has been a reduction in time transferring a patient from the operating theatre to intensive care and a reduction of the number of errors by 50%.
If you want to know more about this you can you view and interview with Martin via the YouTube link.
The YouTube link provided is to Professor Martin Elliott's lecture on his experience with the Formula One team as the interview is no longer available
The Before Action Review helps a team state their intention (task, purpose and end-state) just before commencing the project, project stage or a piece of work, but also adds the discipline of predicting challenges and risks and, most important, drawing on lessons learned from past experiences at the start.
Four questions make up this technique;
- What are we setting out to achieve?
- What can be learned from similar situations and past projects from elsewhere?
- What will deliver success?
- What are the actions we need to take to avoid problems and apply good practice?
It can be run in as little as 15 minutes.
Within appreciative inquiry the focus is on seeing the world differently. Participants are invited to celebrate what is working well, analyse why and then to imagine the best possible future outcome and how to achieve it. The process often involves creative expression of the future outcome.
Think about a recent enquiry you have received or about a key priority for your organisation – could you recommend a learning before tool to help the use of evidence and knowledge?
To get you started think about the following scenarios – how would you introduce a learning before tool
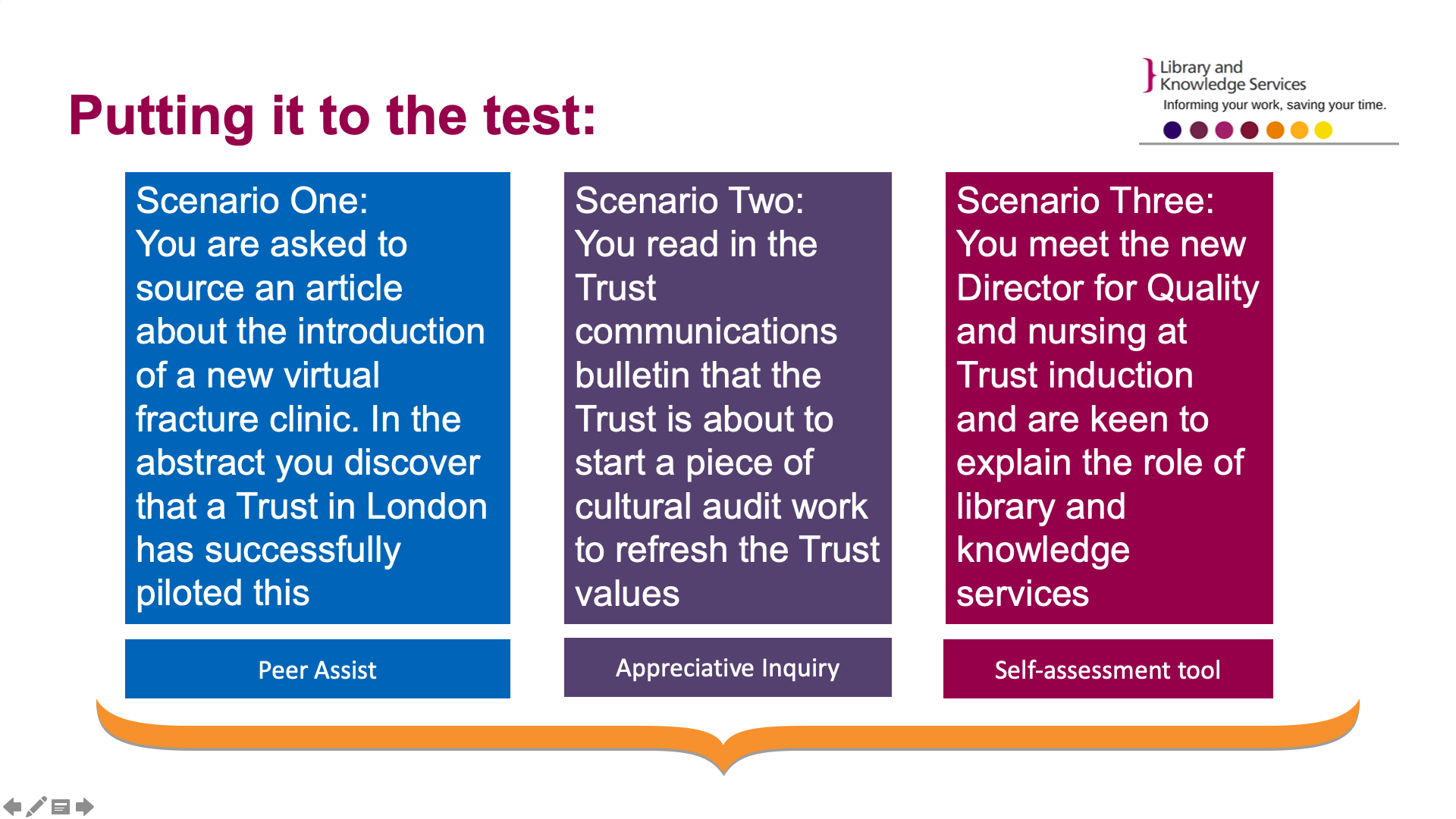
Which learning before tool might you use in the following situations?
In scenario one we imagine that we are supplying an article about new virtual fracture clinics, you notice from the abstract that these have been introduced successfully in a London Trust. What could you share with your requestor to encourage them to learn more?
A Peer Assist will enable one team to learn from another team who have put something similar into place. In this instance you may want to suggest to the person requesting the article that they may like to set up a peer assist with the team from the London Trust to learn more about how they set up the fracture clinic. You could offer to facilitate the session for them.
In scenario 2 you discover that the Trust are planning to refresh the Trust values. What technique could you share with the person leading this work?
Using appreciative inquiry is a great way to encourage people to imagine a positive outcome and would be a good way to engage people to think about Trust values.
In scenario three the new Director for Quality and Nursing visits your stand at Trust induction. Besides inviting him to become a member of the library what knowledge mobilisation technique might you suggest?
Using the self-assessment tool with newly appointed senior staff is a great way to have a conversation about the wide range of services that you can offer and put in place some actions to help them make improve the way they use evidence and knowledge
The next bite sized sessions will explore some of the knowledge mobilisation techniques in more detail, make suggestions for how to get started and provide examples of how they have been used by other knowledge specialists. For further examples visit the KM Toolkit and take a look at the KM stories.
If you would like further information or to share what you have been doing to mobilise evidence and knowledge in your organisation please contact members of the Mobilising Evidence and Knowledge Group.
Page last reviewed: 31 August 2022